|
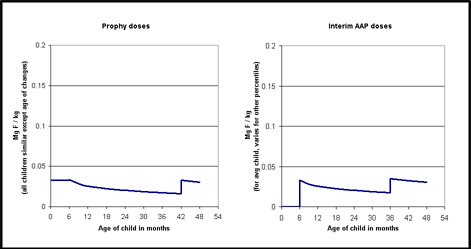
The graph is not very clear, but I think you can get the gist of it.
The main difference between the doses I recommend
(graph on the left) and those of the AAP is the first 6 months. The AAP gives zero, where I give a dose by body weight of
.033 mg F / kg. Later there is a little difference - I switch doses at a body weight and the AAP does it by age.
What
is the significance of these differences? Well, that's hard. Let me first try another graph just to see the differences.
Now let's get back to the significance of the differences. We have not actually tested enough kids for long enough to see
if there are any real differences. The answer I will give is based on theory and a few clinical trials of similar dose schedules
in Europe. (I don't have that data with me, I'll add it in somewhere below.)
Cavities: The 6 month zone of no fluoride
would theoretically cause a slight increase in cavities in the teeth that are forming during that first 6 months. The most
interesting parts of the forming teeth are the tops of front baby teeth (see ECC page) and the chewing surfaces of the first
permanent molars.
White spots: The jumps at each step, especially from zero to .25 mg at age 6 months, would theoretically
cause the pigmentation to shift to a whiter color. These doses are pretty low, so I would not expect a big change, but it
could be barely visible. The position of the change should be a little different than what we have seen from the old doses
when the jump was at birth. It should shift about an eighth of an inch up from the leading edge of the incisors.
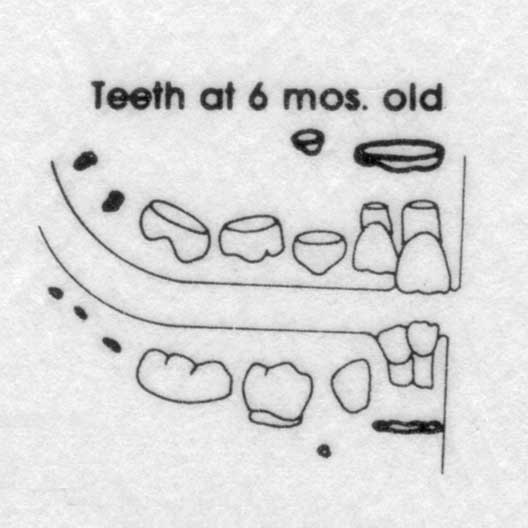
In the drawing above, of the teeth at age six months, you can picture
where the action should be. The permanent teeth are shown in darker, bolder ink. On the permanent central incisors you can
see the part that has just grown. With the old doses (high at birth), this is the part that has mild fluorosis. With the new
doses, the mild fluorosis should be just above this part. In the back teeth you can see the chewing surfaces of the first
permanent molars just forming. The baby teeth have grown quickly, and are just starting to errupt into the mouth.
(This
drawing is adapted from Schour & Massler's classic text on how the teeth grow: Studies in tooth development: the growth
pattern of human teeth. JADA 1940; 27:1778 (part 1) and 1918 (part 2).)
I still don't have the European data at hand,
but let me wing it from memory. (It may be ages before I get around to fixing this.) I think there were three trials of the
zero from birth to 6 months doses. (The rest of the schedules were fairly close to the AAP's , but not exactly like it.)
Two of these trials had only a control group for comparison, but were longer term. I think one found more cavities
(than in different trials of the old .25 mg at birth), and did not look at fluorosis. The other one found no difference in
cavities, even between the F and non-F groups, and lots more fluorosis. (This study was pretty whacko in grouping vast outcomes
together.)
One of the trials was short - to about 5 years of age I think. It compared the zero-until-6-months group
to a group that started at birth. It was a good trial but found no difference in caries. (Rats! But at age 5 most of the exposed
teeth were formed in pregnancy, and we are not quite into enamel that formed with the various F levels.) And the kids weren't
old enough to look for fluorosis yet.
So I have to admit that at this point there is no proven* significance between
starting at birth and at 6 months. So if you already think I am splitting hairs, don't read the next section on "zero start".
I will argue for being even more persnickedy on doses.
* There is now some “proof”, noticed by Dr. Glenn. Cavities are
increasing since the dental lobby got the pediatricians to take
fluoride away from the youngest babies. The report is pretty long and
hairy: http://www.cdc.gov/nchs/data/series/sr_11/sr11_248.pdf
From
it's conclusions: [dental health for almost
everybody has improved, for seniors, adults, adolescents …] “...
However, the prevalence of dental caries in the primary dentition for
youths aged 2–5 years increased from 1988–1994 to 1999–2004.”
(Newborns born after May 1995 started getting no fluoride until age 6
mos.)
|

